
INTRODUCTION
In this article we present the case of a 43-year-old female patient, partial edentulous, with severe case III malocclusion, rotation to the right side and carrying an upper metal ceramic bridge in poor condition, orthognathic surgery and complete upper rehabilitation with zygomatic implants in combination with conventional implants in conjunction with an immediate load prosthesis was proposed to solve the case of malocclusion and partial edentulism.
Nowadays we find more and more cases of patients who demand a fast and effective solution for their tooth loss problems. Often, these patients have severe bone atrophy, so to meet these demands we are forced to offer them other therapeutic alternatives to conventional dental implants with their respective GBR (guided bone regeneration) surgeries, since this type of treatment, despite being reliable and quite predictable, would nowadays take a long time to complete.
In Salud Dental Blanco after several studies, we propose NORIS MEDICAL zygomatic implants, which are the most suitable for the placement of zygomatic implants, for implantation in the extra-sinus malar bone.
Zygomatic implants were introduced to the scientific world by Brånemark in 1998, and since that time changes have been made in both the implants and the procedure, which have led to a considerable decrease in both short and long-term complications.
Traditionally, the atrophic jaw has been treated with autologous, allopathic bone grafts and techniques such as guided bone regeneration and sinus floor elevation.
With zygomatic implants, we are able to offer treatment as reliable as conventional implants and the waiting time is significantly shortened since in most cases we are spared the different existing surgical techniques whose purpose is to increase the amount of bone in the oral cavity. In great maxillary atrophy, we can place zygomatic implants and make immediate loading, something that, in extreme atrophies, without zygomatic implants is practically unthinkable.
CLINICAL CASE


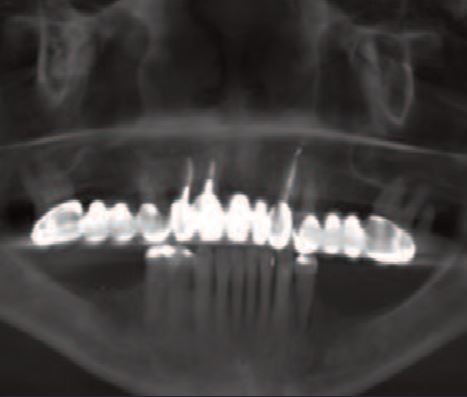
Initial photo and CT scan of the patient, partially edentulous patient, a metal-ceramic bridge of the entire upper part in poor condition along with the teeth that support it.
A 43-year-old woman comes to our clinic with a severe occlusion problem. Severe Class III and hyperplastic atrophy on the right side. Deficit of mobility of the right temporalis muscle.
She underwent a clinical examination, photographs, complete RX series, and CT scan.
The patient has a full upper metal-ceramic bridge, placed many years ago in another clinic, which is now in poor condition along with the teeth that support it.
We plan orthodontic treatment, which will require orthognathic surgery, and later the placement of zygomatic implants in posterior and conventional anterior sectors.
Given the difficulty of performing open sinus lifts for the placement of conventional implants, due to the orthognathic surgery to be performed, together with the demands of the patient to have teeth immediately and not to wait too long to finish the whole treatment, leads us to choose zygomatic implants as the technique of choice for the posterior sectors.
The patient was referred to the maxillofacial surgery service of the Hospital Nuestra Señora de Americ where she underwent upper and lower orthognathic surgery, while she was treated with braces in the antero-inferior sector. After 6 months, and under the authorization of the maxillofacial service, we proceed to perform the implant surgery that we had planned.
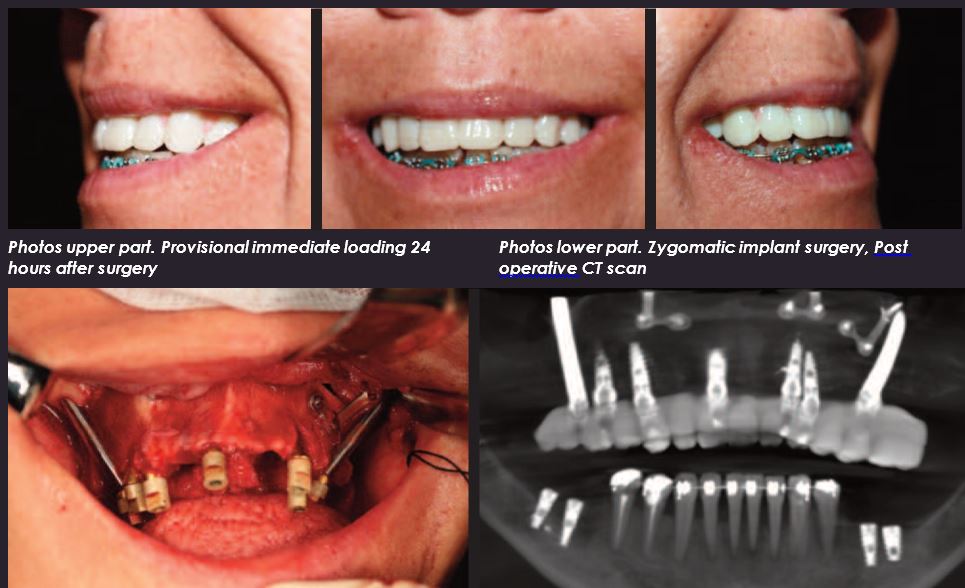
We proceed to the extraction of all the upper pieces and the placement of two zygomatic implants in posterior sectors with five conventional implants in the anterior sector and four more implants in the posterior inferior sectors. All of them are placed with a minimum torque of 40N so we can use the upper implants to support the screw-retained provisional immediate prosthesis that the patient will wear. The patient’s mouth is scanned with Itero and sent to the laboratory where a PMMA prosthesis is manufactured and placed in the patient in less than 24 hours.
We have several alternatives today for the complete rehabilitation of the upper jaw in case of severe atrophy.
Which is the best? The answer is impossible to know since it will depend on many factors and in the end, as long as the result is satisfactory for both the clinician and the patient, we can say that any technique used was optimal for that patient.
In any case, broadly speaking, we can discuss the solution with conventional implants plus bone regeneration techniques and the solution with zygomatic implants.
DISCUSSION
The zygomatic implants depend on the skill of the clinician, since it is not a commonly used technique and not all surgeons know how to perform it, and on the amount of zygomatic bone available to the patient. These implants, within the brand that we have used in this case, have an active part of 4.2 x 13, and the rest of the implant has different measures, adapting the implant to the connection of the zygomatic bone with the maxillary bone. Therefore, in this case, the zygomatic bone had to be sufficient to accommodate two implants of this size on each side.
On the other hand, conventional implants are much easier to place, since their use has become very widespread in recent years, and they have become a conventional treatment.
Even so, for the case in question, the clinician must also have certain skills, since we are talking about cases of large maxillary bone atrophies where the placement of conventional implants cannot be done without prior regenerative techniques of certain complications, such as sinus lifts or even bone distraction
Therefore, the level of skill may be an important point in determining between one technique and another, but it is by no means a determining factor.
On the other hand, we believe that time can be a more determining factor since nowadays, the demands of our patients are increasingly greater. If we place zygomatic implants, we could have the complete rehabilitation finished, with a definitive prosthesis, in 4/5 months, while conventional implants with bone grafts would take longer than that time, only for the graft to osseointegrate.
In addition, the indisputable advantage of being able to wear a fixed temporary prosthesis from the first moment, while, if we perform grafts and conventional implants, the only prosthesis we could use would be a removable one, and not in all cases.

